Newsletter
Where Things Go Wrong
Oct 31, 2017
With a medical malpractice database as big as CRICO’s national comparative benchmarking system (CBS), atypical adverse events become more visible.This is particularly apparent when we look at where the events that prompt allegations of malpractice occur. The clinical specialists who code the CBS cases can choose among more than 60 location codes to identify where the patient was when the triggering event happened.
Claims Made 2007–2016N=56,889 cases, $10.9B incurred losses | ||
Top 10 Locations89% of cases &
| 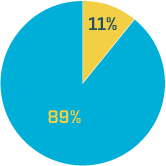 | Other Locations11% of cases & Procedure Settings Pre/Post Treatment Areas Clinical Service Facility |
As we would expect (and the chart illustrates), the vast majority (89%) of casesoccur in the Top 10 locations: settings where the majority of health care isdelivered. But the 11 percent of medmal cases that occur in less common caresettings—or even outside of formal care settings—are spread across more than45 location codes. Even for large health care organizations, the rarity ofcases in any one of these atypical locations may be shielding the need forsome general patient safety education and training. For health care providersand supporting staff in all delivery settings, the perspective enabled by alarger data set may help prevent adverse events where they are leastexpected.
Inthe typical centers of patient care, experience and volume dictate thatadequate staffing, systems, and training be in place to anticipate patientsafety risks and to respond appropriately to an adverse care event. Theroutine exposure to risk generally ensures preparedness essential tointercepting errors, rescuing patients on the precipice of harm, orinitiating rescue/recovery efforts to reduce the impact of a medical mishap.
Butan enterprise-wide commitment to preventing harm ensures that the culture of safetyreaches wherever patients have care encounters (no matter how “minor”), orwhere those patients may end up before or after such encounters. In typicallylow-risk care settings as well as non-clinical locations, staff who are lessattuned to patient safety protocols, and unfamiliar or inadequately trainedfor responding to an emergent adverse event, pose a potential risk topatients’ health and organizational liability. Some level of patient safetyeducation and training is appropriate for everyone who encounters patients.For many clinicians—and most non-clinicians—such training might be their onlyexposure to patient safety, but patients expect to be safe wherever they arereceiving care.
Additional Material
Latest News from CRICO
Postpartum Malpractice Claims: Can We Understand Preventable Harms and Socioeconomic Factors?

Establishing a Regional Registry for Neonatal Encephalopathy: Impact on Identification of Gaps in Practice
The Safety of Inpatient Health Care
