Newsletter
Malpractice Cases Involving Non-Adherent Patients
Apr 02, 2018
As health care has evolved from a paternalist,physician centric model to a team-based, patient-centered model reliant onshared decision making, so too has the terminology used to describe contrarybehavior.
Theterm “difficult” that had been applied to patients who didn’t obey their doctor's orders was first modified to “noncompliant,” then, more recently, to “non-adherent.” Such changes acknowledge patients own the right to follow (i.e., adhere to) or ignore your advice regarding lifestyle choices,treatment regimens, and prescriptions.
What hasn’t changed, however, is clinician angst that they work in a health caredelivery system that limits their ability to convey to patients concerns thattheir decisions or disengagement may pose serious consequences. In a 2011Consumers Report survey of 660 primary care physicians, patient noncompliancewas the top complaint, and that sentiment seems to be increasing.
Timeconstraints, communication barriers, and “Dr. Google” are ubiquitoushindrances. Imparting your recommendations is often a challenge; being ableto engage in a meaningful discussion about why those recommendations matterto the patient’s health is a much bigger challenge. On top of that,clinicians worry that an adverse health outcome will somehow be attributed totheir inability to convince a patient to follow their advice.
Theclinical coders who assign contributing factors to medical malpractice caseshoused in CRICO’s national Comparative Benchmarking System (CBS) recognize that someadverse events are impacted by patient decisions contrary to sound medicaladvice or behavior outside any clinician's influence or control. To capturerelevant instances of non-adherence with recommended treatment, follow up, ormedication regimens, the coders may assign one of the following codes:
- Patient noncompliance with a recommended treatment regimen
- Patient noncompliance with follow-up calls or appointments
- Patient noncompliance with medication(s)
For all CBS cases asserted from 2007–2016, 11 percent had one or more ofthese contributing factors (12 percent of the high-severity cases). Of those,29 percent involve a medical treatment allegation and 23 percent allege adiagnostic failure. Not surprisingly, the vast majority involve outpatientsand primary care providers are the most commonly named.
The presence of these issues does not, of course, suggest that other factors didnot substantially contribute to an adverse outcome, nor do they preclude acase from being brought forth. While the reasons cases are closed with anindemnity payment go far beyond the coded contributing factors, cases that doinclude one or more “patient noncompliance” factor closed with apayment at a rate (25 percent) below the 34 percent rate for all CBScases closed from 2007–2016.
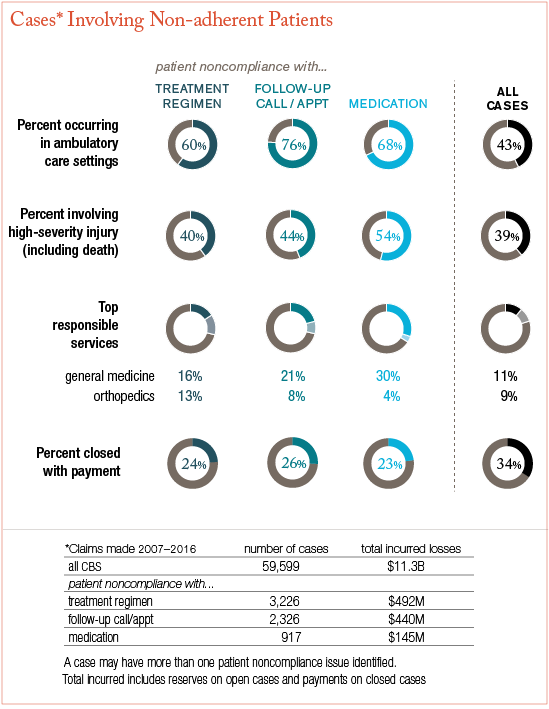
Data for Cases With Non-Adherent Patients: Click to enlarge.
Wary or disengaged patients who have serious health issues will, nevertheless,continue to require and seek care. While non-adherence can be exasperatingwhen you have a broader view of the consequences of such decisions, you mayultimately be able to help those patients by seeing their decisions asdetours rather than dead ends. Probing for the reason a patient rejectstreatment, misses appointments, or neglects medications may expose underlyingissues that you can then address. Reframing the situation (especially forpatients with low health literacy), realignment of expectations, orengagement of family members or social services, are strategies that may helpyour patients make better informed decisions.
Obviously, you can only devote so much time to patients who resist your help. Recordyour education efforts (and materials provided) and document a patient’s refusal of strongly recommended care. If necessary, follow established protocols fortransferring care to another provider. While such actions may not prevent amalpractice claim or lawsuit, they demonstrate your efforts to adequatelyexplain or emphasize the importance of recommended care plans, and to guidethe patient toward appropriate care.
Additional Material
Latest News from CRICO
Ambulatory Safety Nets: Protecting Providers and Promoting Safety with Systems to Reduce Delayed Cancer Diagnoses
